| 5 star | 88% | |
| 4 star | 7% | |
| 3 star | 2% | |
| 2 star | 1% | |
| 1 star | 2% |
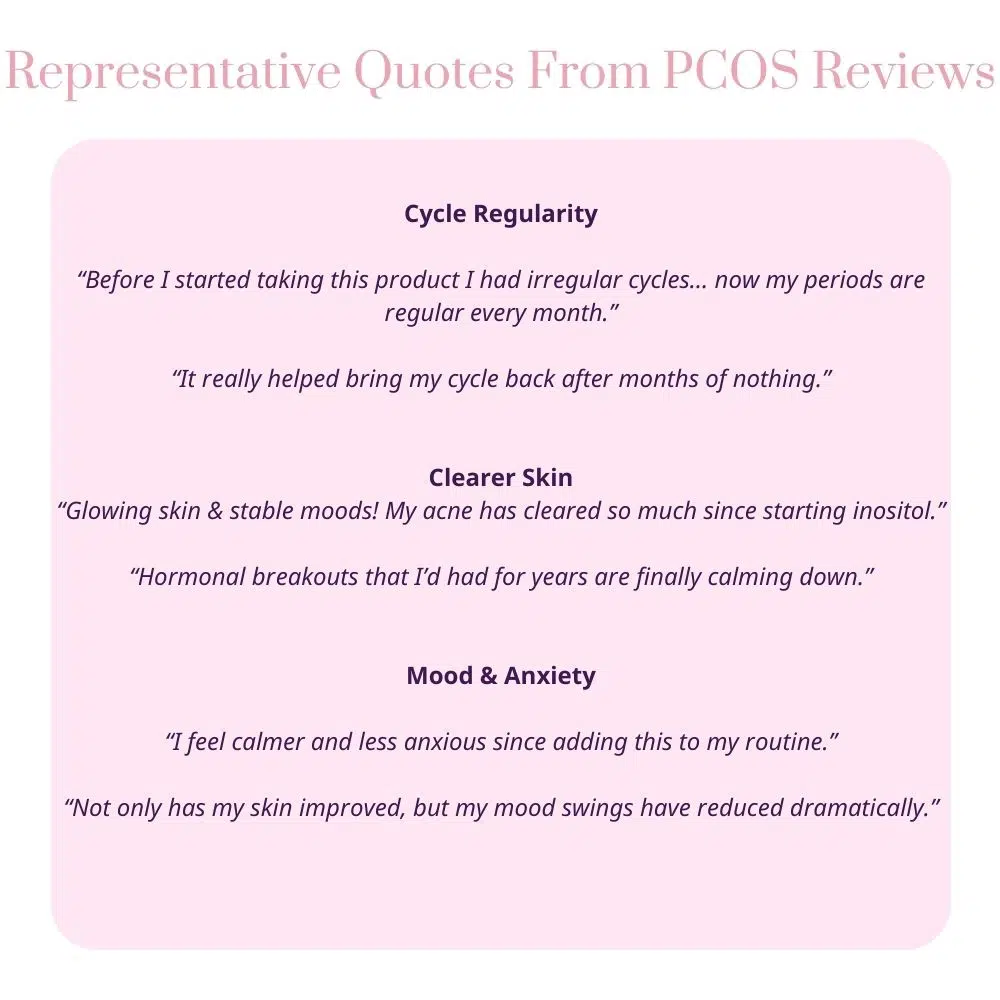
Taking it for a few months, helps with cravings and have a more regular cycle.

Deep into perimenopause, my mood and anxiety are constantly an issue. Since taking inositol my moods are definitely more stable and less irrational, and my nails and hair have improved in strength.
Less symptoms
The issue of PCOS patients over-converting MI to DCI, is identified as a key mechanism underlying the “D-chiro-inositol (DCI) ovarian paradox.”
Here’s what the research reveals:
The report describes how PCOS patients with hyperinsulinemia commonly present “increased levels MI to DCI epimerisation, leading to an MI deficiency in the ovaries, resulting in impaired folliculogenesis, anovulation, and decreased oocyte quality” . This over-conversion is mediated by insulin-stimulated epimerase activity, where “insulin can stimulate enzymatic activity in the ovaries, leading to an increase in the DCI/MYO conversion rate” .
The research emphasises that different tissues have vastly different inositol requirements. The physiological ovarian MI/DCI ratio is 100:1, which is “much higher” than the serum ratio of 40:1, “with a greater need for MI due to its role in FSH signaling” . This suggests that ovaries are particularly vulnerable to MI deficiency when conversion rates increase.
Multiple studies describe what’s termed the “D-chiro-Ins ovarian paradox” . In PCOS ovaries, “increased epimerase activity leads to local Myo-Ins deficiency” which “may adversely affect glucose uptake and metabolism of both oocytes and follicular cells” . This creates a situation where the ovary becomes depleted of the specific inositol form it needs most.
The research provides clinical evidence that this over-conversion is problematic. Isabella et al. demonstrated that “increasing DCI dosage progressively worsens oocyte quality and ovarian response” in non-insulin-resistant PCOS patients . This suggests that adding more DCI (the end product of conversion) when conversion is already excessive can further harm ovarian function.
The over-conversion has specific functional consequences because MI and DCI serve different roles: “MI increases glucose cellular uptake and D-chiro-Ins is involved in glycogen synthesis” . Since ovaries require glucose uptake for proper function rather than glycogen storage, the shift toward DCI production impairs ovarian metabolism.
This over-conversion research suggests that PCOS treatment should focus on restoring MI availability rather than providing more DCI. The research indicates that “myo-inositol treatment rather than D-chiro-inositol is able to improve oocyte and embryo quality during ovarian stimulation protocols” in euglycemic PCOS patients , supporting the idea that correcting MI deficiency is more important than adding DCI. The research comprehensively addresses this over-conversion issue as a central mechanism explaining why standard 40:1 ratios may be inappropriate for many PCOS patients, particularly those undergoing fertility treatments.
Based on the research report, here are the key citations specifically relating to the over-conversion paradox:
V. Unfer et al., 2016 – This is the most comprehensive source, describing:
O. Pustotina et al., 2024 – Provides detailed mechanistic explanation:
R. Isabella et al., 2012 – Describes the clinical paradox:
N. Mendoza et al., 2017 – Supports the conversion mechanism:
V. Unfer et al., 2011 – Provides clinical evidence of the paradox effects in euglycemic PCOS patients undergoing ICSI
M. Nordio et al., 2019 – Shows that “too much DCI causes a loss of beneficial effects at the reproductive level”
Here’s the simple, gentle overview of changes many women notice in the first 3 months of taking myo-inositol for PCOS:
– You might not notice big changes right away, and that’s totally okay.
– Some people feel a slight boost in energy or steadier mood as blood sugar regulation begins to improve.
– Mild digestive adjustments can happen but usually settle quickly if you start with a lower dose and build up.
– Many women start to see improvements in menstrual cycle regularity or spotting a bit more predictable timing.
– Some notice fewer cravings or less intense sugar dips.
– Skin may start to feel calmer, though acne improvements often take longer.
– Ovulation may become more regular—this can sometimes be tracked with ovulation kits or basal body temperature if you’re monitoring fertility.
– Energy levels often feel more stable throughout the day.
– Hormonal symptoms like excess hair growth or acne might begin to soften, but these changes can take more time and may need additional approaches.
– Overall sense of feeling more balanced and in tune with your body is common.
Remember, everyone’s body is unique. Some see faster changes, others more gradual. It’s about gentle progress and tuning in to what feels different for you.
You Can track your changes using this Inositol 12 Week Progress Checker worksheet.
Many women with PCOS find acne frustrating, as it’s often linked to hormonal imbalances—especially elevated androgens like testosterone—that can increase oil production and clog pores.
Myo-Inositol does help to improve skin condition. It was reported in 65% of reviews from women with PCOS when we analysed the data on inositol benefits.
Preliminary scientific evidence suggests that myo-inositol supplementation may help improve acne in women with PCOS, likely through improvements in insulin sensitivity and reduced androgen levels, though the current evidence base lacks rigorous methodology and quantitative outcome data needed for definitive conclusions.
Here’s how myo-inositol might help with acne in PCOS:

It’s important to remember:
Two studies examining myo-inositol supplementation for acne in women with PCOS were identified, both reporting improvements in acne-related outcomes following 6 months of treatment. The Ciotta et al. study demonstrated significant improvement in acne scores compared to placebo, while the Pezza et al. study found significant improvements in acne-related quality of life measures (CADI and DLQI) at 3 and 6 months. Both studies also reported improvements in insulin sensitivity, with the Pezza study additionally demonstrating reductions in testosterone and DHEAS levels, providing a plausible mechanistic pathway for acne improvement through reduced hyperandrogenism.
However, the evidence remains preliminary. Neither study provided quantitative baseline or post-treatment acne severity data, standardized acne grading scales were not clearly specified, and only abstracts were available for review. The Pezza study used a combination product containing magnesium and folic acid alongside myo-inositol, complicating attribution of effects. While the consistent direction of benefit across studies and favorable safety profile (no adverse events reported) suggest myo-inositol may be a reasonable adjunctive option for PCOS-related acne, definitive conclusions await randomized controlled trials with validated acne outcome measures.
(2012). M043 MYO‐INOSITOL VS D‐CHIRO INOSITOL IN PCOS TREATMENT. Minerva Ginecologica