
Final batch now shipping. Limited Stock Remaining. ⏳ Dismiss
Skip to content


The issue of PCOS patients over-converting MI to DCI, is identified as a key mechanism underlying the “D-chiro-inositol (DCI) ovarian paradox.”
Here’s what the research reveals:
The report describes how PCOS patients with hyperinsulinemia commonly present “increased levels MI to DCI epimerisation, leading to an MI deficiency in the ovaries, resulting in impaired folliculogenesis, anovulation, and decreased oocyte quality” . This over-conversion is mediated by insulin-stimulated epimerase activity, where “insulin can stimulate enzymatic activity in the ovaries, leading to an increase in the DCI/MYO conversion rate” .
The research emphasises that different tissues have vastly different inositol requirements. The physiological ovarian MI/DCI ratio is 100:1, which is “much higher” than the serum ratio of 40:1, “with a greater need for MI due to its role in FSH signaling” . This suggests that ovaries are particularly vulnerable to MI deficiency when conversion rates increase.
Multiple studies describe what’s termed the “D-chiro-Ins ovarian paradox” . In PCOS ovaries, “increased epimerase activity leads to local Myo-Ins deficiency” which “may adversely affect glucose uptake and metabolism of both oocytes and follicular cells” . This creates a situation where the ovary becomes depleted of the specific inositol form it needs most.
The research provides clinical evidence that this over-conversion is problematic. Isabella et al. demonstrated that “increasing DCI dosage progressively worsens oocyte quality and ovarian response” in non-insulin-resistant PCOS patients . This suggests that adding more DCI (the end product of conversion) when conversion is already excessive can further harm ovarian function.
The over-conversion has specific functional consequences because MI and DCI serve different roles: “MI increases glucose cellular uptake and D-chiro-Ins is involved in glycogen synthesis” . Since ovaries require glucose uptake for proper function rather than glycogen storage, the shift toward DCI production impairs ovarian metabolism.
This over-conversion research suggests that PCOS treatment should focus on restoring MI availability rather than providing more DCI. The research indicates that “myo-inositol treatment rather than D-chiro-inositol is able to improve oocyte and embryo quality during ovarian stimulation protocols” in euglycemic PCOS patients , supporting the idea that correcting MI deficiency is more important than adding DCI. The research comprehensively addresses this over-conversion issue as a central mechanism explaining why standard 40:1 ratios may be inappropriate for many PCOS patients, particularly those undergoing fertility treatments.
Based on the research report, here are the key citations specifically relating to the over-conversion paradox:
V. Unfer et al., 2016 – This is the most comprehensive source, describing:
O. Pustotina et al., 2024 – Provides detailed mechanistic explanation:
R. Isabella et al., 2012 – Describes the clinical paradox:
N. Mendoza et al., 2017 – Supports the conversion mechanism:
V. Unfer et al., 2011 – Provides clinical evidence of the paradox effects in euglycemic PCOS patients undergoing ICSI
M. Nordio et al., 2019 – Shows that “too much DCI causes a loss of beneficial effects at the reproductive level”
We recommend a dose of 4g per day taken as 2g in the morning with breakfast and 2g taken in the evening with dinner.
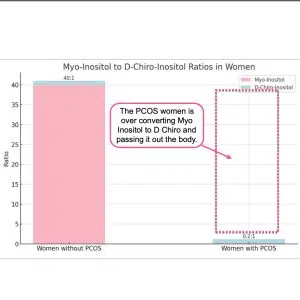
The inositol problem in PCOS is that the body over converts Myo Inositol (MI) into D Chiro Inositol. (DCI) Adding more DCI isn’t the answer.
In PCOS patients with hyperinsulinemia, increased epimerase activity leads to excessive conversion of MI to DCI in the ovary, resulting in MI depletion and DCI overproduction (Nestler & Unfer, 2015; Unfer et al., 2014).
This imbalance may impair FSH signaling and oocyte quality (Nestler & Unfer, 2015). Studies have shown that the MI:DCI ratio in follicular fluid drops from 100:1 in healthy women to 0.2:1 in PCOS patients (Unfer et al., 2014).
The altered MI:DCI ratio may contribute to pathological steroidogenesis in PCOS, with DCI promoting androgen synthesis and reducing estradiol production (Unfer et al., 2020).
Restoring the appropriate MI:DCI ratio has shown efficacy in PCOS treatment, and MI supplementation may improve oocyte and sperm quality in assisted reproduction (Facchinetti et al., 2016).
In addition D-Chiro has negative long term effects.
Please read:
Nordio, M.; Bezerra Espinola, M.S.; Bilotta, G.; Capoccia, E.; Montanino Oliva, M. Long-Lasting Therapies with High Doses of D-chiro-inositol: The Downside. J.Clin. Med. 2023, 12, 390. https://doi.org/10.3390/jcm12010390
R. GAMBIOLI, G. FORTE, C. ARAGONA, A. BEVILACQUA, M. BIZZARRI, V. UNFER. The use of D-chiro-Inositol in clinical practice European Review for Medical and Pharmacological Sciences 2021; 25: 438-446
The 40:1 ratio contains 2.5-fold more d-chiro-inositol than the physiological ovarian requirement (100:1), creating relative DCI excess that impairs oocyte quality, increases FSH requirements, and can block aromatase activity—making it suboptimal for fertility outcomes particularly in assisted reproduction, despite effectiveness for restoring ovulation in insulin-resistant anovulatory patients.
The available evidence suggests the 40:1 myo-inositol to d-chiro-inositol (MI/DCI) ratio demonstrates context-dependent efficacy rather than being universally “wrong” for PCOS and fertility. The ratio appears effective for restoring ovulation in anovulatory, insulin-resistant patients seeking natural conception, but multiple lines of evidence indicate it may be suboptimal for oocyte quality during assisted reproduction. Head-to-head comparisons consistently favor MI over DCI for fertility outcomes in ART contexts, with Isabella et al. demonstrating dose-dependent deterioration in oocyte quality, embryo quality, and FSH requirements as DCI doses increase from 300 to 2400 mg. Mechanistically, the physiological ovarian MI/DCI ratio is 100:1—approximately 2.5-fold higher than the 40:1 ratio used in supplements—suggesting the 40:1 formulation contains excessive DCI relative to ovarian tissue requirements. The “D-chiro-inositol ovarian paradox” explains that increased epimerase activity in PCOS ovaries already creates local MI deficiency, which exogenous DCI at 40:1 may exacerbate rather than correct. Furthermore, high DCI doses can block aromatase expression and paradoxically cause hyperandrogenism, potentially impairing fertility despite systemic metabolic benefits. However, the evidence does not conclusively prove 40:1 is wrong for all PCOS patients: it may represent an acceptable compromise for anovulation when systemic insulin sensitization is needed, but appears excessive for euglycemic patients or those prioritizing oocyte quality in assisted reproduction, where ratios approaching the physiological 100:1 may be preferable.
Read the full report here: Why 40:1 myo-inositol to d-chiro Inositol is wrong for PCOS and Fertility
(2012). CONCERN: Does ovary need D-chiro-inositol?. Journal of Ovarian Research
Myo-inositol begins restoring ovulation within 3-5 weeks but achieves optimal pregnancy rates after 3-6 months of sustained treatment.
Myo-inositol demonstrates a hierarchical timeline of fertility effects, with the earliest measurable responses occurring within 1 week. Estradiol concentrations increased within the first week of treatment, representing the initial hormonal response. Functional ovulatory restoration occurred more gradually, with time to first ovulation at 24.5 days (95% CI: 18-31 days) compared to 40.5 days for placebo, and 88% of PCOS women experiencing their first spontaneous menstrual cycle after a mean of 34.6±5.5 days. Clinical pregnancies required sustained treatment, with large observational cohorts documenting 70% ovulation restoration and 15.1% pregnancy rates by 10.2 weeks, while extended 6-month protocols achieved 40% pregnancy rates. Significant hormonal changes, including testosterone reduction and progesterone elevation, were consistently documented after 12 weeks.
The optimal treatment duration depends on therapeutic context. For women seeking spontaneous conception, treatment should be sustained for 3-6 months to maximize pregnancy outcomes, while ovulatory effects become apparent within 4-5 weeks. For IVF protocols, 1-2 months of pre-treatment improved oocyte quality and fertilization rates. However, most studies were not designed with timing as a primary endpoint, and only one trial provided confidence intervals for time-to-event outcomes. The evidence suggests a dose-response relationship between treatment duration and pregnancy rates, though individual response varies based on baseline characteristics such as BMI
Full research report here: How long does it take for myo-inositol to work for fertility.
E. Papaleo, V. Unfer, J. Baillargeon, L. De Santis, F. Fusi, and 5 more