
Final batch now shipping. When it’s gone, orders close. ⏳ Dismiss
Skip to content


The issue of PCOS patients over-converting MI to DCI, is identified as a key mechanism underlying the “D-chiro-inositol (DCI) ovarian paradox.”
Here’s what the research reveals:
The report describes how PCOS patients with hyperinsulinemia commonly present “increased levels MI to DCI epimerisation, leading to an MI deficiency in the ovaries, resulting in impaired folliculogenesis, anovulation, and decreased oocyte quality” . This over-conversion is mediated by insulin-stimulated epimerase activity, where “insulin can stimulate enzymatic activity in the ovaries, leading to an increase in the DCI/MYO conversion rate” .
The research emphasises that different tissues have vastly different inositol requirements. The physiological ovarian MI/DCI ratio is 100:1, which is “much higher” than the serum ratio of 40:1, “with a greater need for MI due to its role in FSH signaling” . This suggests that ovaries are particularly vulnerable to MI deficiency when conversion rates increase.
Multiple studies describe what’s termed the “D-chiro-Ins ovarian paradox” . In PCOS ovaries, “increased epimerase activity leads to local Myo-Ins deficiency” which “may adversely affect glucose uptake and metabolism of both oocytes and follicular cells” . This creates a situation where the ovary becomes depleted of the specific inositol form it needs most.
The research provides clinical evidence that this over-conversion is problematic. Isabella et al. demonstrated that “increasing DCI dosage progressively worsens oocyte quality and ovarian response” in non-insulin-resistant PCOS patients . This suggests that adding more DCI (the end product of conversion) when conversion is already excessive can further harm ovarian function.
The over-conversion has specific functional consequences because MI and DCI serve different roles: “MI increases glucose cellular uptake and D-chiro-Ins is involved in glycogen synthesis” . Since ovaries require glucose uptake for proper function rather than glycogen storage, the shift toward DCI production impairs ovarian metabolism.
This over-conversion research suggests that PCOS treatment should focus on restoring MI availability rather than providing more DCI. The research indicates that “myo-inositol treatment rather than D-chiro-inositol is able to improve oocyte and embryo quality during ovarian stimulation protocols” in euglycemic PCOS patients , supporting the idea that correcting MI deficiency is more important than adding DCI. The research comprehensively addresses this over-conversion issue as a central mechanism explaining why standard 40:1 ratios may be inappropriate for many PCOS patients, particularly those undergoing fertility treatments.
Based on the research report, here are the key citations specifically relating to the over-conversion paradox:
V. Unfer et al., 2016 – This is the most comprehensive source, describing:
O. Pustotina et al., 2024 – Provides detailed mechanistic explanation:
R. Isabella et al., 2012 – Describes the clinical paradox:
N. Mendoza et al., 2017 – Supports the conversion mechanism:
V. Unfer et al., 2011 – Provides clinical evidence of the paradox effects in euglycemic PCOS patients undergoing ICSI
M. Nordio et al., 2019 – Shows that “too much DCI causes a loss of beneficial effects at the reproductive level”
Here’s the simple, gentle overview of changes many women notice in the first 3 months of taking myo-inositol for PCOS:
– You might not notice big changes right away, and that’s totally okay.
– Some people feel a slight boost in energy or steadier mood as blood sugar regulation begins to improve.
– Mild digestive adjustments can happen but usually settle quickly if you start with a lower dose and build up.
– Many women start to see improvements in menstrual cycle regularity or spotting a bit more predictable timing.
– Some notice fewer cravings or less intense sugar dips.
– Skin may start to feel calmer, though acne improvements often take longer.
– Ovulation may become more regular—this can sometimes be tracked with ovulation kits or basal body temperature if you’re monitoring fertility.
– Energy levels often feel more stable throughout the day.
– Hormonal symptoms like excess hair growth or acne might begin to soften, but these changes can take more time and may need additional approaches.
– Overall sense of feeling more balanced and in tune with your body is common.
Remember, everyone’s body is unique. Some see faster changes, others more gradual. It’s about gentle progress and tuning in to what feels different for you.
You Can track your changes using this Inositol 12 Week Progress Checker worksheet.
Many women with PCOS find acne frustrating, as it’s often linked to hormonal imbalances—especially elevated androgens like testosterone—that can increase oil production and clog pores.
Myo-Inositol does help to improve skin condition. It was reported in 65% of reviews from women with PCOS when we analysed the data on inositol benefits.
Preliminary scientific evidence suggests that myo-inositol supplementation may help improve acne in women with PCOS, likely through improvements in insulin sensitivity and reduced androgen levels, though the current evidence base lacks rigorous methodology and quantitative outcome data needed for definitive conclusions.
Here’s how myo-inositol might help with acne in PCOS:

It’s important to remember:
Two studies examining myo-inositol supplementation for acne in women with PCOS were identified, both reporting improvements in acne-related outcomes following 6 months of treatment. The Ciotta et al. study demonstrated significant improvement in acne scores compared to placebo, while the Pezza et al. study found significant improvements in acne-related quality of life measures (CADI and DLQI) at 3 and 6 months. Both studies also reported improvements in insulin sensitivity, with the Pezza study additionally demonstrating reductions in testosterone and DHEAS levels, providing a plausible mechanistic pathway for acne improvement through reduced hyperandrogenism.
However, the evidence remains preliminary. Neither study provided quantitative baseline or post-treatment acne severity data, standardized acne grading scales were not clearly specified, and only abstracts were available for review. The Pezza study used a combination product containing magnesium and folic acid alongside myo-inositol, complicating attribution of effects. While the consistent direction of benefit across studies and favorable safety profile (no adverse events reported) suggest myo-inositol may be a reasonable adjunctive option for PCOS-related acne, definitive conclusions await randomized controlled trials with validated acne outcome measures.
(2012). M043 MYO‐INOSITOL VS D‐CHIRO INOSITOL IN PCOS TREATMENT. Minerva Ginecologica
We can’t offer medical advice, but here’s how many women with PCOS say inositol—especially myo‑inositol—can support their day-to-day wellbeing.
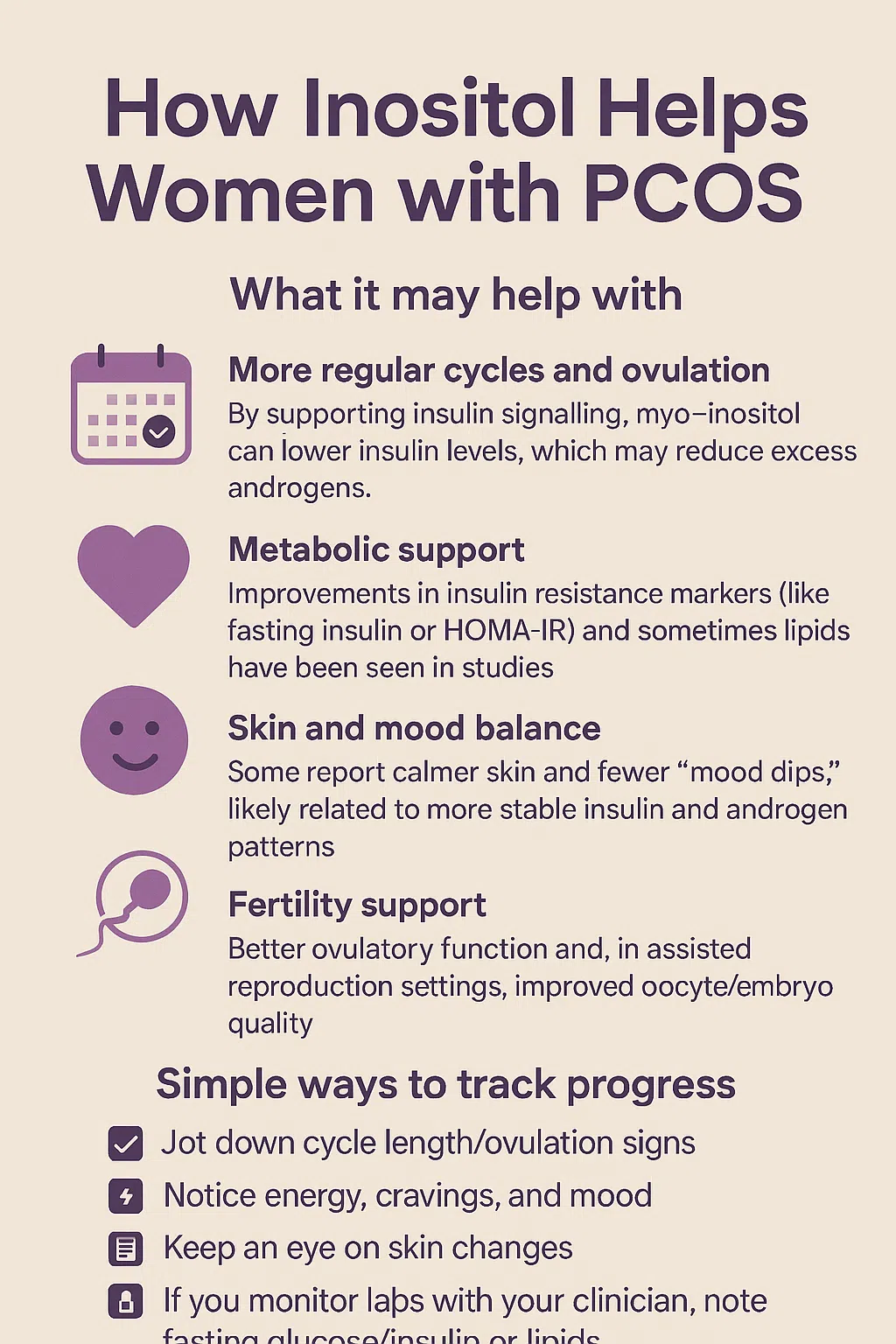
What it may help with
Safety and what to expect
Simple ways to track progress
Key references (plain‑language summaries available if helpful)
You can read our own analysis of over 400 real reviews here.
Refer to the Evidence Based Guidelines & our 12 essential PCOS blood tests post for more details on this.
✅ Anti-Müllerian Hormone (AMH)
✅ Total and Free Testosterone or Free Androgen Index (FAI)
✅ DHEAS (Dehydroepiandrosterone Sulfate)
✅ Sex Hormone-Binding Globulin (SHBG)
✅ Prolactin
✅ LH, FSH, and Estradiol (optional, not diagnostic)
✅ TSH (Thyroid-Stimulating Hormone)
✅ Free T4 (if thyroid dysfunction suspected)
✅ Oral Glucose Tolerance Test (OGTT)
✅ HbA1c
✅ Fasting insulin and glucose (for HOMA-IR)
✅ Lipid Profile (Total Cholesterol, LDL, HDL, Triglycerides)
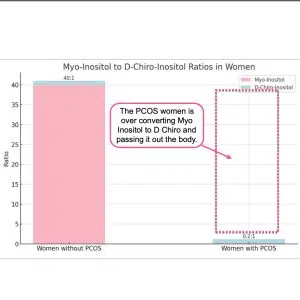
The inositol problem in PCOS is that the body over converts Myo Inositol (MI) into D Chiro Inositol. (DCI) Adding more DCI isn’t the answer.
In PCOS patients with hyperinsulinemia, increased epimerase activity leads to excessive conversion of MI to DCI in the ovary, resulting in MI depletion and DCI overproduction (Nestler & Unfer, 2015; Unfer et al., 2014).
This imbalance may impair FSH signaling and oocyte quality (Nestler & Unfer, 2015). Studies have shown that the MI:DCI ratio in follicular fluid drops from 100:1 in healthy women to 0.2:1 in PCOS patients (Unfer et al., 2014).
The altered MI:DCI ratio may contribute to pathological steroidogenesis in PCOS, with DCI promoting androgen synthesis and reducing estradiol production (Unfer et al., 2020).
Restoring the appropriate MI:DCI ratio has shown efficacy in PCOS treatment, and MI supplementation may improve oocyte and sperm quality in assisted reproduction (Facchinetti et al., 2016).
In addition D-Chiro has negative long term effects.
Please read:
Nordio, M.; Bezerra Espinola, M.S.; Bilotta, G.; Capoccia, E.; Montanino Oliva, M. Long-Lasting Therapies with High Doses of D-chiro-inositol: The Downside. J.Clin. Med. 2023, 12, 390. https://doi.org/10.3390/jcm12010390
R. GAMBIOLI, G. FORTE, C. ARAGONA, A. BEVILACQUA, M. BIZZARRI, V. UNFER. The use of D-chiro-Inositol in clinical practice European Review for Medical and Pharmacological Sciences 2021; 25: 438-446
Inositol is a very safe food supplement. It is naturally found in mothers breast milk and often used in infant formulas and baby foods.
For a small percentage of women there is an adjustment process. This may mean headaches, dizziness, stomach ache or more frequent urination for the first few days or even weeks.
If this is the case for you, then we recommend you take your regular over the counter headache tablets and or start on a smaller dose and build up to the recommended dose slowly.
So rather than 4 grams per day you might take 1g in week 1, 2g in week 2, 3g in week 3, 4g in week 4.
It may also be helpful to split the daily dose into a morning and evening serving.
If problems persist stop taking inositol immediately and talk to your GP.
Inositol is recommended by some GP’s to women who are pregnant as it reduces the risk of gestational diabetes.
There are a number of peer reviewed studies where there has been no adverse effects from near conception through to delivery.
Always check with your GP if this is right for you.
We have not found a study to say that inositol in breastmilk causes problems for breastfeeding infants.
There are studies to support some positive benefits but there isn’t a lot of research on this.
We recommend that you make your own searches using the above provided sources.
If you do find something that we haven’t seen please let us know.
The recommended daily dose for women with PCOS is 4 grams per day. This can be taken as 1 x 4g dose in the morning. Or as 2g with breakfast in the morning and 2g in the evening with dinner.A 4 gram serve is a not quite flat metric teaspoon. A 2 gram serve is a not quite flat metric 1/2 teaspoon. We now provide a 2g scoop in our Natural Myo Inositol Product.
It is recommended that you don’t take inositol with a lot of coffee as too much caffeine reduces the positive benefits. There isn’t a negative health effect rather just the reduction of positive effects.
How much is a lot? Depends on your body size and other factors but 3+ cups of coffee a day is a good place to start.
The planting area for corn in Australia averages 160,000 hectares and produces around 440,000 tonnes.
In China the area planted for corn is 76,000,000 acres producing 257 million tonnes.
This is well over 500 times more corn grown than in Australia.
Inositol production is a small fraction of this large quantity.
We haven’t found an Australian grown Inositol supply and suspect that the Australian industry is too small and serves other higher yield markets
It makes total sense to want a clear, simple way to explain PCOS—especially because it can feel confusing and a bit overwhelming when you’re living it. You’re doing a really good thing by getting informed and bringing your partner into it. It has effects on partners in the relationship, not just yourself.
PCOS (Polycystic Ovary Syndrome) is a very common hormone condition that affects how the ovaries work.
Here’s the simplest way to describe it:
1) “My ovaries have lots of follicles, but they don’t always release an egg”
People with PCOS often, but not always, have many small follicles (tiny “egg sacs”) in the ovaries.
They can look like “cysts” on an ultrasound, but they aren’t usually true cysts—it’s more like the ovaries are “stocked up,” and the eggs don’t mature and release as regularly.
What that can feel like day-to-day: periods that are irregular, unpredictable, or missing.
2) “Ovulation can be irregular—so timing is harder”
Because ovulation (releasing an egg) may happen less often or unpredictably, cycles can be longer or inconsistent.
This is one reason PCOS can make it harder to conceive, not because pregnancy is impossible, but because ovulation is harder to predict.
3) “Insulin resistance is often part of the picture”
A lot of people with PCOS have insulin resistance, meaning the body needs more insulin than usual to manage blood sugar. Higher insulin can then nudge the ovaries to make more androgens (hormones like testosterone).
What that can feel like: energy dips, intense cravings, feeling “wired then tired,” or trouble feeling stable between meals (everyone’s experience varies).
4) “Higher androgens can show up in visible ways”
Those higher androgens can contribute to things like:
5) “It can affect mood too—and it’s not ‘all in your head’”
Living with fluctuating hormones, fatigue, and uncertainty can affect mood, anxiety, motivation, and self-confidence. That’s a real part of PCOS for many people.
“PCOS is a hormone condition where my ovaries don’t always release an egg regularly. That can make my periods unpredictable and can affect fertility timing. A lot of PCOS is linked to insulin resistance, which can also affect energy and cravings. It’s manageable, but it’s a real physical thing—not just stress—and support helps.”
Gentle, grounded reassurance
PCOS is common (often cited around 6–15% of reproductive-age women, depending on criteria), and there are multiple ways to support it—usually starting with lifestyle foundations, and sometimes medication or targeted supplements with a clinician’s guidance.
For in depth review we suggest you look at Teede HJ, et al. International evidence-based guideline for the assessment and management of PCOS (2018; updated 2023). Human Reproduction / Monash University guideline group.
Yes. It is GMO Free, Plant Based and Vegan safe. It is made from corn.
Depends on advice from your doctor. We cannot give medical advice and this is even more specialised as it is a toxicology question relating to your personal circumstances which we are not qualified to know.