

The issue of PCOS patients over-converting MI to DCI, is identified as a key mechanism underlying the “D-chiro-inositol (DCI) ovarian paradox.”
Here’s what the research reveals:
The Over-Conversion Problem
The report describes how PCOS patients with hyperinsulinemia commonly present “increased levels MI to DCI epimerisation, leading to an MI deficiency in the ovaries, resulting in impaired folliculogenesis, anovulation, and decreased oocyte quality” . This over-conversion is mediated by insulin-stimulated epimerase activity, where “insulin can stimulate enzymatic activity in the ovaries, leading to an increase in the DCI/MYO conversion rate” .
Tissue-Specific Requirements
The research emphasises that different tissues have vastly different inositol requirements. The physiological ovarian MI/DCI ratio is 100:1, which is “much higher” than the serum ratio of 40:1, “with a greater need for MI due to its role in FSH signaling” . This suggests that ovaries are particularly vulnerable to MI deficiency when conversion rates increase.
The Paradox Mechanism
Multiple studies describe what’s termed the “D-chiro-Ins ovarian paradox” . In PCOS ovaries, “increased epimerase activity leads to local Myo-Ins deficiency” which “may adversely affect glucose uptake and metabolism of both oocytes and follicular cells” . This creates a situation where the ovary becomes depleted of the specific inositol form it needs most.
Clinical Evidence of Over-Conversion Effects
The research provides clinical evidence that this over-conversion is problematic. Isabella et al. demonstrated that “increasing DCI dosage progressively worsens oocyte quality and ovarian response” in non-insulin-resistant PCOS patients . This suggests that adding more DCI (the end product of conversion) when conversion is already excessive can further harm ovarian function.
Functional Consequences
The over-conversion has specific functional consequences because MI and DCI serve different roles: “MI increases glucose cellular uptake and D-chiro-Ins is involved in glycogen synthesis” . Since ovaries require glucose uptake for proper function rather than glycogen storage, the shift toward DCI production impairs ovarian metabolism.
Treatment Implications
This over-conversion research suggests that PCOS treatment should focus on restoring MI availability rather than providing more DCI. The research indicates that “myo-inositol treatment rather than D-chiro-inositol is able to improve oocyte and embryo quality during ovarian stimulation protocols” in euglycemic PCOS patients , supporting the idea that correcting MI deficiency is more important than adding DCI. The research comprehensively addresses this over-conversion issue as a central mechanism explaining why standard 40:1 ratios may be inappropriate for many PCOS patients, particularly those undergoing fertility treatments.
Based on the research report, here are the key citations specifically relating to the over-conversion paradox:
Primary References for the Over-Conversion Paradox:
V. Unfer et al., 2016 – This is the most comprehensive source, describing:
- The “D-chiro-Ins ovarian paradox” concept
- How increased epimerase activity in PCOS ovaries leads to local MI deficiency
- Tissue-specific ratios (100:1 in ovary vs 40:1 in serum)
- How reduced intraovarian MI affects glucose uptake and oocyte metabolism
O. Pustotina et al., 2024 – Provides detailed mechanistic explanation:
- How hyperinsulinemic patients present “increased levels MI to DCI epimerization”
- The physiological ovarian ratio being 100:1 vs serum 40:1
- Warning that “high doses and prolonged DCI use can block aromatase expression and lead to hyperandrogenism”
R. Isabella et al., 2012 – Describes the clinical paradox:
- Proposes the “D-chiro-inositol paradox in the ovary of PCOS patients”
- Explains how PCOS patients with hyperinsulinemia have “enhanced MI to DCI epimerization rate in the ovary”
- Shows that “MI depletion could eventually be responsible for the poor oocyte quality”
N. Mendoza et al., 2017 – Supports the conversion mechanism:
- Documents how “insulin can stimulate enzymatic activity in the ovaries, leading to an increase in the DCI/MYO conversion rate”
- Notes “contradictory results on DCI effectiveness in ovarian tissue”
Supporting Evidence:
V. Unfer et al., 2011 – Provides clinical evidence of the paradox effects in euglycemic PCOS patients undergoing ICSI
M. Nordio et al., 2019 – Shows that “too much DCI causes a loss of beneficial effects at the reproductive level”
Research has not yet evaluated whether myo-inositol can balance hormones in healthy people without PCOS or fertility issues.
Myo-inositol—typically given at 2–4 g daily in combination with 200–400 μg folic acid—has been shown to improve ovarian parameters in women with polycystic ovary syndrome. In non‐PCOS women undergoing in vitro fertilization, one study reported that myo-inositol reduced gonadotropin requirements (2,084 ± 648 IU versus 2,479 ± 979 IU, p < 0.05) and modified luteinizing hormone levels (2.7 ± 1.1 vs. 1.6 ± 0.9, p < 0.01) while yielding fewer oocytes (5.9 ± 2.4 vs. 7.6 ± 3.8, p < 0.01) and producing no significant differences in pregnancy or implantation rates. No study has evaluated hormone balancing effects in healthy, non-infertile populations outside of the assisted reproduction setting. Mild gastrointestinal side effects have been noted at higher doses, although no substantial safety concerns were reported.
Myo-Inositol for Hormonal Balance – Report
References
Lisi, F., Carfagna, P., Oliva, M., Rago, R., Lisi, R., Poverini, R., Manna, C., Vaquero, E., Caserta, D., Raparelli, V., Marci, R., & Moscarini, M. (2012). Pretreatment with myo-inositol in non polycystic ovary syndrome patients undergoing multiple follicular stimulation for IVF: a pilot study. Reproductive Biology and Endocrinology, 10(1), 52. https://doi.org/10.1186/1477-7827-10-52
Laganà, A. S., Vitagliano, A., Noventa, M., Ambrosini, G., & D’Anna, R. (2018). Myo-inositol supplementation reduces the amount of gonadotropins and length of ovarian stimulation in women undergoing IVF: a systematic review and meta-analysis of randomized controlled trials. Archives of Gynecology and Obstetrics, 298(4), 675–684. https://doi.org/10.1007/s00404-018-4861-y
Sortino, M. A., Salomone, S., Carruba, M. O., & Drago, F. (2017). Polycystic Ovary Syndrome: Insights into the Therapeutic Approach with Inositols. Frontiers in Pharmacology, 8. https://doi.org/10.3389/fphar.2017.00341
Gerli, S., Papaleo, E., Ferrari, A., & Renzo, G. D. (2007). Randomized, double blind placebo-controlled trial: effects of myo-inositol on ovarian function and metabolic factors in women with PCOS. European Review for Medical and Pharmacological Sciences.
F. R. C. “Computer S., Academy, I. S. M., V.I. Kulakov Research Center of Obstetrics, G. and P., & Academy, I. S. M. (2018). Myo-inositol: micronutrient for “fine tuning” of the female reproductive sphere. LLC Russian Medical Journal. https://doi.org/10.32364/2618-8430-2018-1-2-148-155
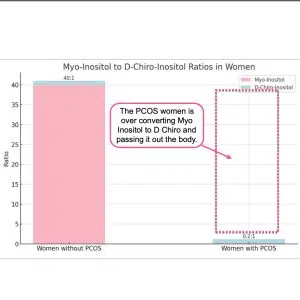
The inositol problem in PCOS is that the body over converts Myo Inositol (MI) into D Chiro Inositol. (DCI) Adding more DCI isn’t the answer.
In PCOS patients with hyperinsulinemia, increased epimerase activity leads to excessive conversion of MI to DCI in the ovary, resulting in MI depletion and DCI overproduction (Nestler & Unfer, 2015; Unfer et al., 2014).
This imbalance may impair FSH signaling and oocyte quality (Nestler & Unfer, 2015). Studies have shown that the MI:DCI ratio in follicular fluid drops from 100:1 in healthy women to 0.2:1 in PCOS patients (Unfer et al., 2014).
The altered MI:DCI ratio may contribute to pathological steroidogenesis in PCOS, with DCI promoting androgen synthesis and reducing estradiol production (Unfer et al., 2020).
Restoring the appropriate MI:DCI ratio has shown efficacy in PCOS treatment, and MI supplementation may improve oocyte and sperm quality in assisted reproduction (Facchinetti et al., 2016).
In addition D-Chiro has negative long term effects.
Please read:
Nordio, M.; Bezerra Espinola, M.S.; Bilotta, G.; Capoccia, E.; Montanino Oliva, M. Long-Lasting Therapies with High Doses of D-chiro-inositol: The Downside. J.Clin. Med. 2023, 12, 390. https://doi.org/10.3390/jcm12010390
R. GAMBIOLI, G. FORTE, C. ARAGONA, A. BEVILACQUA, M. BIZZARRI, V. UNFER. The use of D-chiro-Inositol in clinical practice European Review for Medical and Pharmacological Sciences 2021; 25: 438-446
If you have PCOS then give them a copy of the 2023 PCOS Evidence Based Guidelines here. Secondly ask them to look at the research papers linked here. (two tabs in a spreadsheet.) Thirdly ask them to create an account with elicit.org and do some research themselves.
They are all the same ingredient – natural GMO free Myo Inositol. The dose differs between PCOS, Fertility, IR (4g /day) and Cognitive Health (15g/day). Also FAQs, Blog Posts and Reviews are divided by use category to make it easier to find relevant information. Post purchase support information is also divided by use.
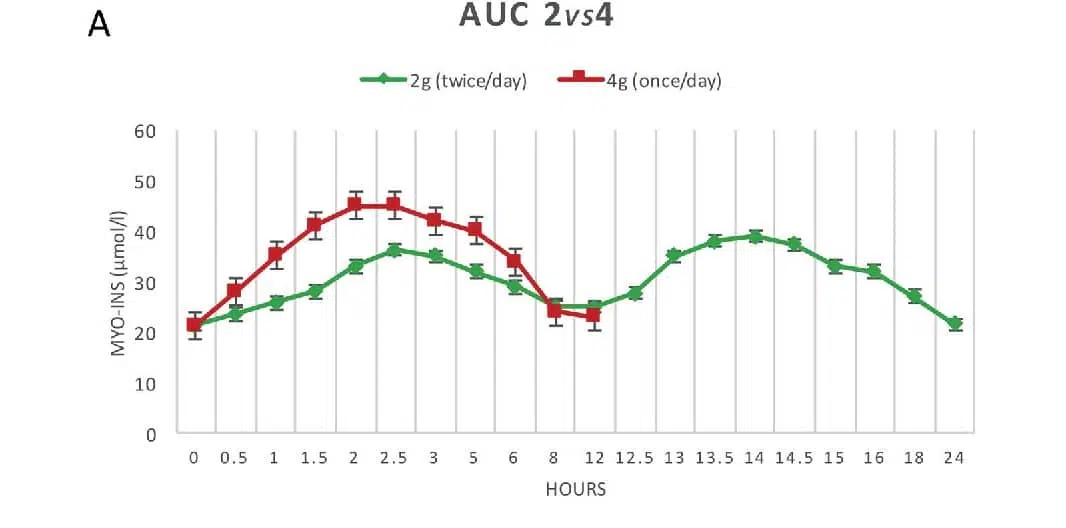
It has been studied and the recommended approach is 2g in the morning and 2g in the evening to get a full 24 hour effect.
Refer to
Finding the best therapeutic approach for PCOS: the importance of inositol(s)bioavailability.
- B. OrrùR. CircoG. Carlomagno
- Published 1 June 2017
- European review for medical and pharmacological sciences.
Our Myo Inositol does not contain ethyl alcohol and is Halal certified.

Inositol is a type of carbohydrate that is found in small amounts in various foods, including grains, fruits, and nuts. The product on this site is a dietary supplement made from corn.
In-os-it-ol



What are the benefits of using Myo-Inositol Powder
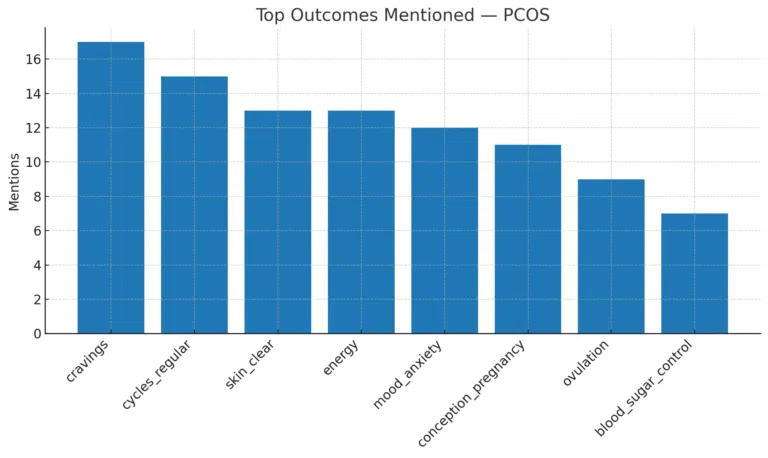
Inositol Australia: Real PCOS & fertility insights from verified reviews. Myo-Inositol powder boosts ovulation, energy, blood sugar control & wellbeing.

Essential PCOS Blood Tests: Your Quick Guide
Essential PCOS blood tests: thyroid function, OGTT, HbA1c and lipid profile for heart health and hormonal balance in Australia.
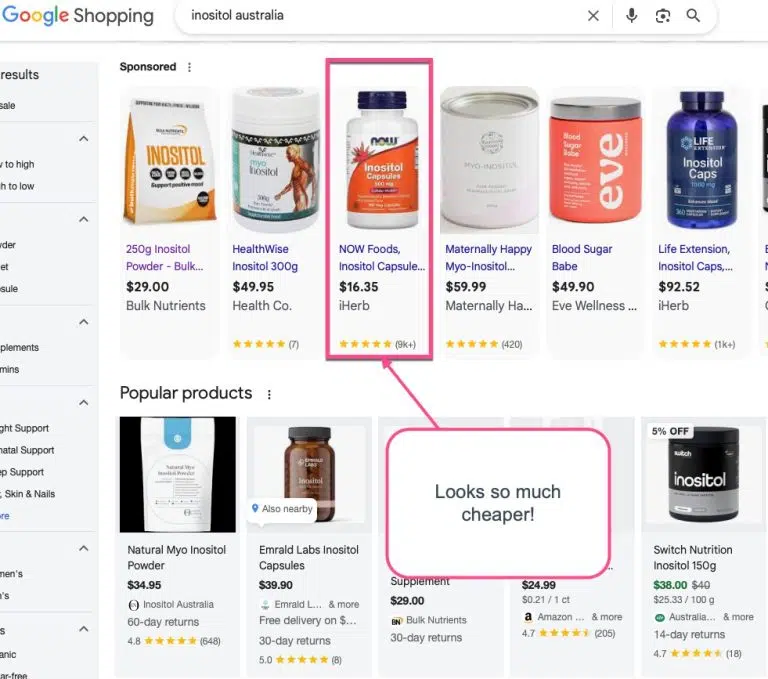
Inositol Capsules vs Powder: Australia Price & Pros
Inositol Australia: Capsules vs Powder — save more with powder, mix into coffee or smoothies, TGA-listed NF-USP grade, cheapest online.